
Audio By Carbonatix
Laboratory medicine is central to modern healthcare, underpinning a substantial proportion of clinical decision-making. The accuracy, timeliness, and interpretive value of laboratory results directly influence diagnosis, treatment, and patient outcomes. As diagnostic technologies evolve, so too have debates about governance, professional roles, and leadership within laboratory systems. In Ghana, these debates must be situated within a broader global discourse on how best to structure diagnostic services for efficiency, quality, and patient safety.
International experience demonstrates that tensions over laboratory control are neither new nor unique to Ghana. In the United Kingdom, reforms within the National Health Service clarified the distinction between biomedical scientists' operational roles and pathologists' clinical responsibilities. In the United States, regulatory frameworks such as the Clinical Laboratory Improvement Amendments emphasise competency-based leadership rather than exclusive professional ownership. Similarly, South Africa's National Health Laboratory Service operates a hybrid model integrating pathologists, scientists, and technologists within a unified governance structure. Across these systems, the consistent principle is functional differentiation and collaborative governance, not hierarchical control.
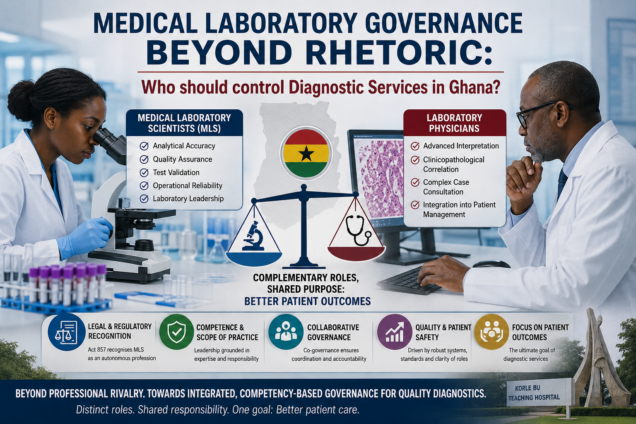
At the core of Ghana's debate lies a conceptual misunderstanding of laboratory practice. Modern laboratory medicine operates across two interdependent domains: the analytical and the clinical. Medical Laboratory Scientists (MLS) ensure analytical accuracy, quality assurance, and operational reliability across all testing phases. Laboratory physicians, by contrast, focus on advanced interpretation, clinicopathological correlation, and integration of results into patient management. These roles are complementary rather than hierarchical. High-quality diagnostic services depend on their coordinated interaction, not professional dominance.
This distinction becomes clearer in practice. MLS professionals manage routine and complex analytical processes, including test validation, quality control, and technical consultation. Their expertise ensures reliability in investigations such as haematology, clinical chemistry, and infectious disease diagnostics. Laboratory physicians contribute primarily in complex scenarios requiring interpretive depth, such as malignancy diagnosis or transfusion complications. Effective governance must therefore align responsibility with functional expertise.
Importantly, the competency profile of MLS professionals has evolved significantly. Training now incorporates molecular diagnostics, laboratory informatics, quality systems, and translational research, supported by postgraduate education and specialist certification through bodies such as the West African Postgraduate College of Medical Laboratory Science. This evolution reflects a global shift toward scientifically specialised, systems-driven laboratory practice. The contemporary MLS is thus equipped not only for technical roles but also for leadership in laboratory governance and quality management.
Ghana's legal framework reinforces this position. The Health Professions Regulatory Bodies Act, 2013 (Act 857) recognises Medical Laboratory Science as an autonomous profession regulated by the Allied Health Professions Council. MLS practitioners are legally accountable for generating, validating, and assuring the quality of diagnostic data. This statutory recognition underscores a key principle: leadership within laboratory systems should be grounded in competence and defined scope of practice, not professional title alone. International standards such as ISO 15189 further assign responsibility for quality systems, validation, and continuous improvement to trained laboratory professionals - core MLS competencies.
The ongoing dispute at Korle Bu Teaching Hospital illustrates the tension between historical structures and contemporary realities. While laboratory services were historically pathology-led, advances in training, regulation, and technology have shifted practice toward competency-based models. The current conflict is therefore less about individual appointments and more about an unresolved transition in governance philosophy. Framing it as a contest for control risks obscuring the underlying need for structural reform.
Claims that MLS leadership constitutes "scope creep" are similarly misplaced. Laboratory medicine is inherently interdisciplinary, and MLS professionals are not seeking to assume clinical roles but to exercise authority within their technical domain. Equally, assertions regarding patient safety must be evidence-based. There is limited empirical support for the notion that physician-led laboratories are inherently safer. On the contrary, safety outcomes are determined by the robustness of quality systems, adherence to standards, and clarity of roles. In this regard, many MLS-led laboratories in Ghana have achieved international accreditation through quality improvement programmes aligned with global benchmarks.
A more sustainable approach lies in adopting a co-governance model. Under such a framework, MLS professionals lead laboratory operations, quality management, and workflow systems, while laboratory physicians provide clinical oversight, advanced interpretation, and consultative input in complex cases.
Governance structures, such as management boards and multidisciplinary teams, ensure coordination, accountability, and continuous improvement. This model reflects international best practice and aligns with the realities of resource-constrained health systems, where specialist capacity must be strategically deployed.
Ultimately, the question is not which profession should control laboratory services, but how governance can best support patient care. Diagnostic systems function optimally when authority is aligned with expertise, roles are clearly defined, and collaboration is institutionalised. In Ghana, moving beyond professional contestation toward a competency-based, integrated governance framework is essential. The strength of medical laboratory practice lies not in hierarchy, but in coordinated expertise, anchored in mutual respect, recognition of distinct professional mandates, functional autonomy, regulatory clarity, and a shared commitment to diagnostic quality and patient outcomes.
The writer, Emmanuel Akomanin Asiamah is a Faculty Member, Department of Medical Laboratory Sciences, University of Health and Allied Sciences (UHAS), Ho, and Consultant Medical Laboratory Scientist, Ho Teaching Hospital, Ghana.
Latest Stories
-
Appeals Court judgement speaks to tremendous flaws – Prof. Gyampo says corruption fight cannot survive prosecutorial incompetence
12 minutes -
Bole-Bamboi MP Yusif Sulemana thanks well-wishers after earning PhD in Business Administration
19 minutes -
15 suspected galamseyers arrested near Obuasi school after viral video exposes site
24 minutes -
Court of Appeal ignored ‘mountain of evidence’ in Sedina’s acquittal – Alfred Tuah-Yeboah
25 minutes -
Minority Leader criticises government over governance, economy and tribunal law
27 minutes -
Unemployed Graduates with Disabilities give government one-week ultimatum over GES recruitment
28 minutes -
Akim Swedru MP slams COCOBOD Act over restrictions on cocoa farmers’ land use
30 minutes -
Mahama cites viral ‘Buz Stop Boys’ video to urge better sanitation practices
33 minutes -
Fuel prices could change daily as Bulk Oil Distributors abandon fixed pricing model
36 minutes -
Minority criticises Minerals Commission over alleged ‘shoddy’ mining leases
36 minutes -
NPP gears up for Oti Regional Elections with 219 accredited delegates
38 minutes -
The Law 101: Burden of Proof, Defective Charges, and Constitutional Safeguards -Sedina Christine Tamakloe Attionu v. The Republic (Suit No: H2/17/2026)
39 minutes -
Ghana’s 24-Hour economy needs strong foundations to deliver – Prof. Amoah
41 minutes -
When they come for you, send them to me – Sam Jonah’s message to new UCC Vice-Chancellor
44 minutes -
Stop talking down Ghana; have faith in the nation’s future – Mahama to Ghanaians
44 minutes